


Source: Supra-Gingival Minimally Invasive Dentistry: A Healthier Approach to Esthetic Restorations, published by Wiley-Blackwell
As any clinician knows, patients come in for esthetic dental treatment not just so that their teeth look better, but for their smile and entire face to improve. They want “big picture” results. Because of this, it’s important that we keep in mind dentofacial esthetics, which is the evaluation of teeth as they relate to facial symmetry and facial structures.
The first step to ensure a harmonious dentofacial outcome when multiple anterior teeth are being planned for treatment, should be a dentofacial evaluation and design. And while esthetics are always subjective, there are some basic parameters.
Parameter, Not Rules
Blending the patient’s goals and preferences with known esthetic parameters can consistently give you results that are predictable and that patients are satisfied with.
Before the smile diagnosis can be completed, information that can be used for diagnosis must be gathered and presented to the patient.
The following records should be completed by a well-trained dental assistant (local laws may limit their duties):
- A full set of periapical x-rays
- A panoramic x-ray (not required but highly recommended)
- Six-point periodontal charting
- Articulated casts mounted using a face bow and a semi-adjustable articulator.
- A series of 11 high-quality photographs, which can be completed with a simple point-and-shoot digital camera.
Through a series of forms and communication, the dentofacial esthetic diagnosis system takes the clinician step by step, guiding with principles, but not absolute rules, to allow for individual preference.
Some important parameters apply in this process — both clinical parameters for ensuring a healthy occlusion and esthetic parameters that are universal definitions of beauty.
Smile Design Step By Step
The 11 simple photographs taken by the dental assistant should be displayed on the computer screen(or printed), allowing the patient to observe the different views of their own smile. All findings should be recorded on the dentofacial esthetic diagnosis form.
The parameters of dentofacial esthetics are best illustrated through photos, and each view and parameters will be assessed. Some questions to reflect on are:
- If the parameter is within acceptable limits. If so, it is not necessary to discuss with the patient.
- If the problem be corrected with restorative dentistry. If so, explain the specific treatment to the patient, including their options, and the estimated cost to correct. If it is not correctable, explain the limitations; or suggest a specialist (orthodontist, periodontist, oral surgeon).
Usually only a few parameters, typically five or six, will need to be discussed. In most cases, the entire smile design procedure should take approximately 10-15 minutes.
25 Parameters (part 1)
The following are general guidelines for each of the dentofacial parameters, not rules. The patient’s preference, willingness to proceed with corrective treatment, and budget will matter significantly when discussing these parameters.
1 Occlusal Plane, Front Full-Face Smiling

Figure 1: (a) Canted occlusal plane. (b) Form with correction notes. (c) After occlusal cant correction with veneers.
Take an imaginary line parallel to the horizon and touch the incisal edges of both centrals and either the incisal edge of the canines or equidistant to both canines, laterals and the rest of the dentition.
2 Midline (Front Full-Face Smiling)

Figure 2: (a) Midline discrepancy, canted midline. (b) Supragingival minimally invasive veneer preparation. (c) Improved midline and esthetics 5 years postoperatively.
The midline is a vertical line that dissects the face vertically and can use glabella (the point where the nose and forehead connect), philtrum, or cupid’s bow, as a facial reference. The facial midline and the dental midline should ideally coincide, but they often do not. If the midline is perpendicular to the occlusal plane, the dental midline can be up to 2 mm off-center and the human eye will barely detect the disparity.
3 Facial Symmetry (Front Full-Face Smiling)
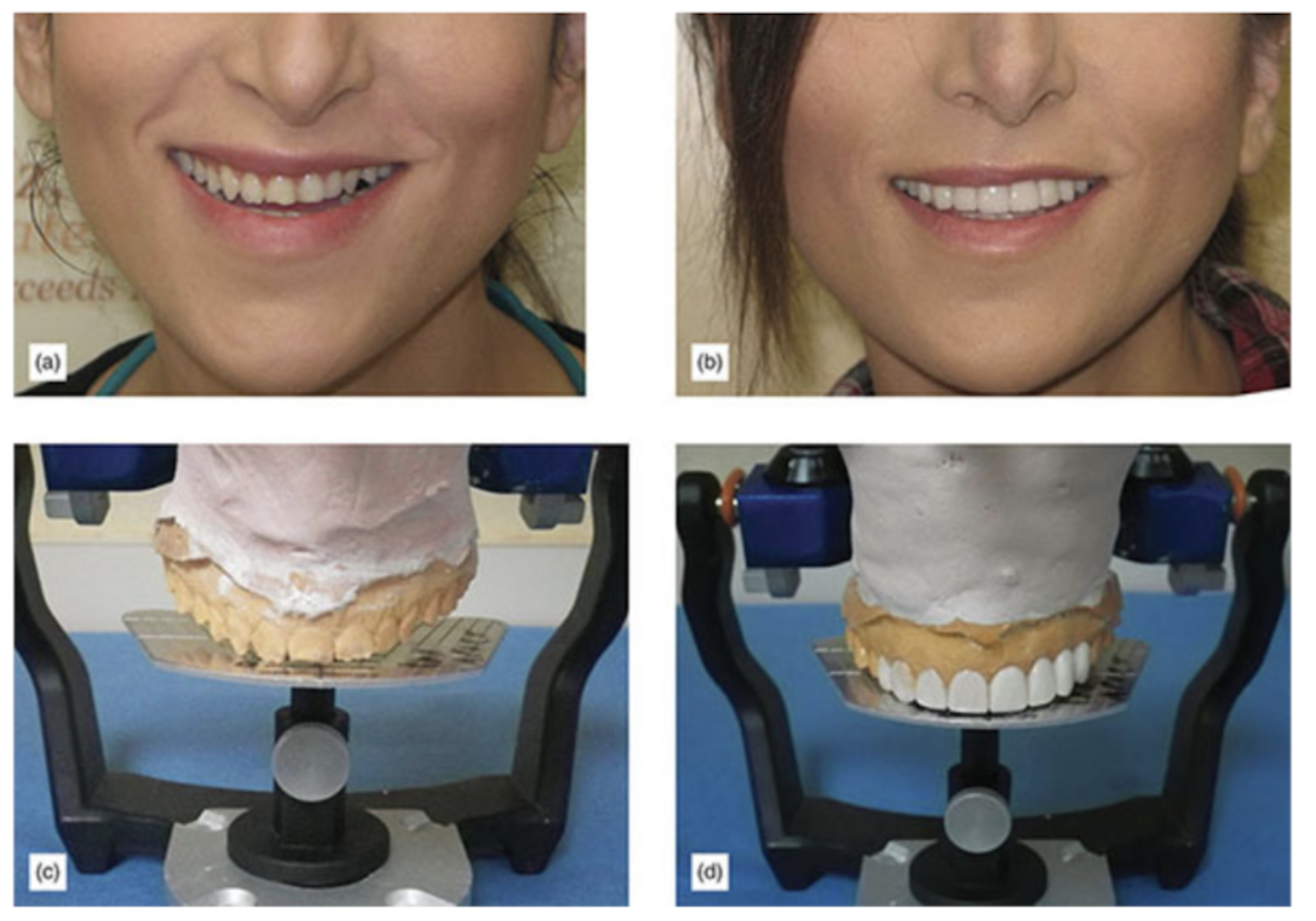
Figure 3: (a) Facial asymmetries will compromise diagnosis and final results, and must be discussed in advance to avoid unreasonable expectations. (b) Excellent results, still showing the complexity of correcting asymmetrical faces/smiles. (c) Facebow-mounted cast, using a diagnostic plate calibrated with the facebow and articulator. (d) Wax-up showing corrected midline and occlusal plane (at the prototype stage).
Facial asymmetries can throw off the occlusal plane and midline. They can also greatly complicate the evaluation and communication with the laboratory, which may lead to compromised results. Good communication with the laboratory and acceptable corrections will only be possible by the correct use of a calibrated facebow mounted cast.
4 Lip Position (Profile)

Figure 4: Cephalometry shows the lip being supported by the teeth.
As the lips are supported by the teeth, changes in dental protrusion will have an effect on the look of the lips, whether positive or negative. So it is important to consider the lip position and lip support.
Ricketts E-line is an imaginary line drawn between the tip of the nose and tip of the chin. The upper lip should be 1 mm from the line and the lower lip should touch it. As this parameter is subjective and dependent on ethnicity, the patient’s opinion should be the primary guideline.
5 Facial Lower Third (Profile view)

Figure 5: Collapsed lower third, compared after bite opening with a full upper arch rehabilitation.
The lower facial third collapses primarily because of the lack of posterior teeth to support the vertical dimension of occlusion and because of severe occlusal wear. This can have an aging effect. As improvement can be very rejuvenating, when orthodontic or extensive restorative treatment is being planned, this parameter should be considered.
6 Tooth Show (Front Smile View)
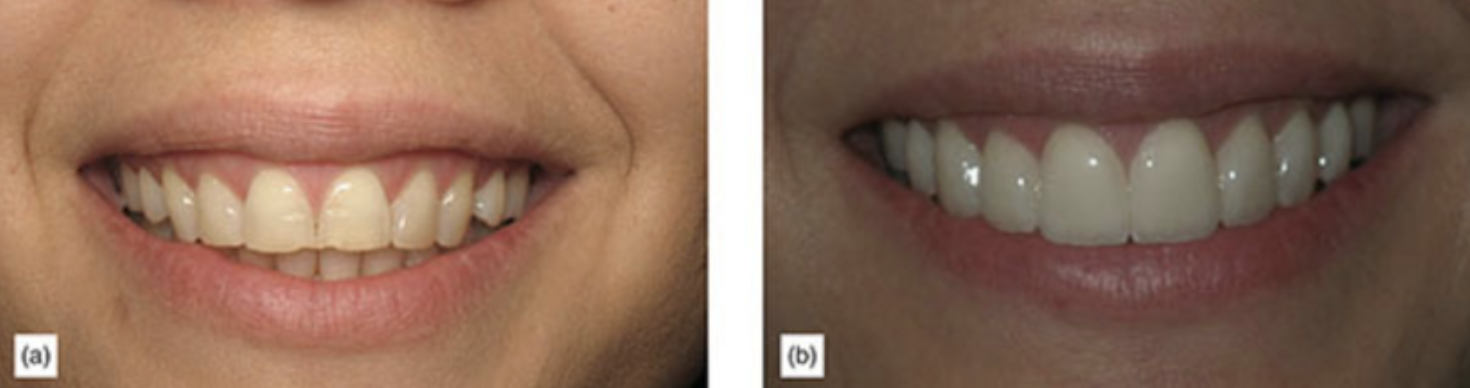
Figure 6: (a) Short anterior teeth due to incisal wear caused by occlusal disease. (b) Porcelain veneers with increased length, creating a more youthful appearance.
Tooth show is often one of the most considered parameters by the patient. Their goals and preferences are crucial during the evaluative process. It is also an age-defining parameter, and when teeth have severe wear, some incisal edge lengthening will have a rejuvenating effect on the smile. Ideally, the incisal edge of the maxillary teeth should be close to touching the lower lip. The further away from the upper teeth are from the lip and the more lower tooth is visible during the smile, the older the smile will look.
7 Buccal Corridor (Front Smile View)
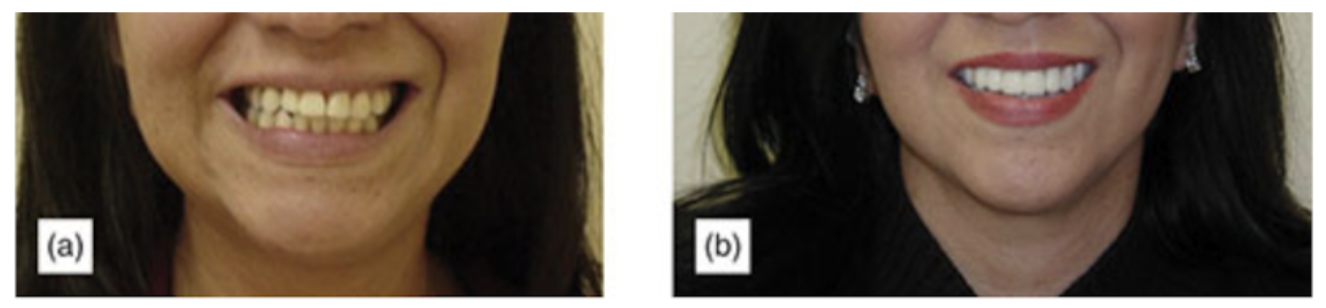
Figure 7: (a) Asymmetrical buccal corridor problem. (b) Corrected buccal corridor.
A desire to have wide arches and little buccal corridor shadow or space guides the buccal corridor parameter. Orthodontics with extracted bicuspids usually lead to a collapsed or narrow maxillary arch, although sometimes narrow arches are a natural occurrence. Restorative or orthodontic options can be discussed with the patient if during the evaluation the patient wished to have a fuller smile.
8 Gingival Show (Front Smile View)
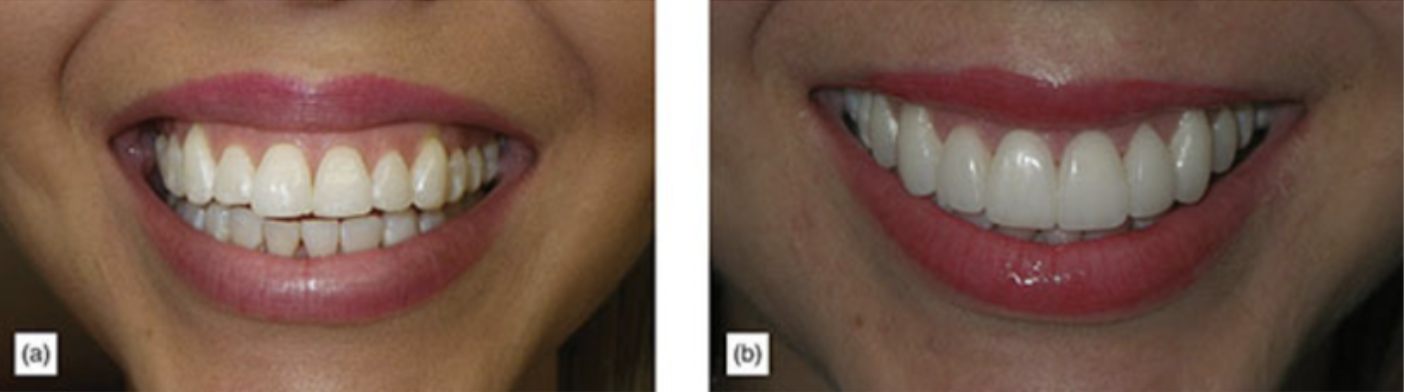
Figure 8: (a) Excessive and asymmetrical gingival display. (b) After crown lengthening surgery and porcelain veneers.
A gingival display is any gingiva that shows above the crown zenith of the teeth. The amount of gingiva displayed should be bilaterally symmetrical. Generally, up to 2 mm of display is acceptable for most women, but because men generally have longer lips, any amount of gingival display is not esthetically pleasing. Crown lengthening surgery can usually correct a “gummy smile.”
9 Incisal Plane (Front Smile View)
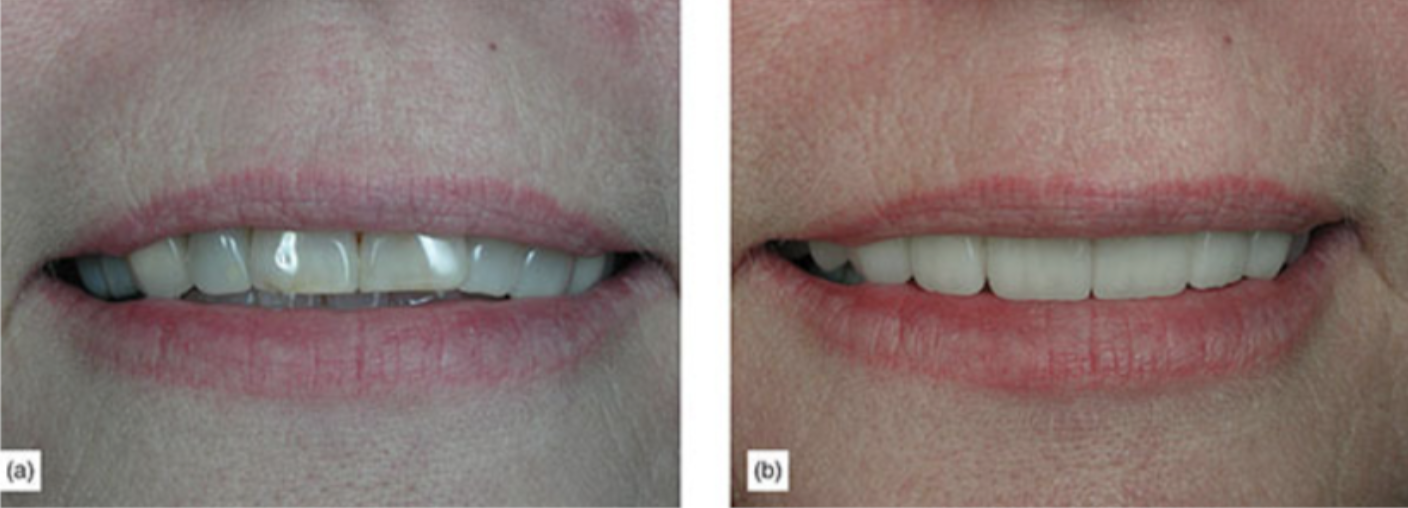
Figure 9: (a) Reverse curve. (b) After correction with veneers.
The incisal plane, a line which touches the incisal edges of all visible teeth, should be continuous and should have a positive curvature, like a happy face. Reverse, irregular, or wavy curves are undesirable.
10 Incisal Plane to Lip (Front Smile View)

Figure 10: Incisal plane following lip curvature.
It is desirable for the incisal edge to follow the curvature of the lower lip. Lips have different curvatures and ignoring the type of lip curvature can lead to unesthetic results.
11 Conversational Tooth Show
Some systems suggest taking a view with the lip in repose, to help to determine the appropriate amount of tooth show. It is, however, more important to know how much tooth shows when the patient is speaking, as this is the time when the teeth are being observed by others (Figures 11a,b,12a,b). A conversational display can be recorded by taking pictures while the patient repeats the number “66.” In a similar way to the amount of tooth visible when smiling, the amount of conversational tooth show decreases with age.
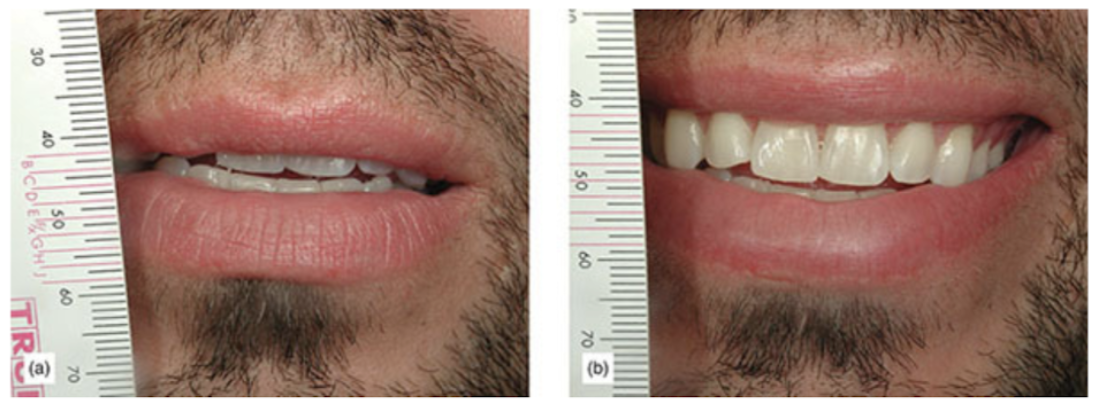
Figure 11: (a) Male repeating the number “66,” a conversational tooth view. (b) Same male smiling.
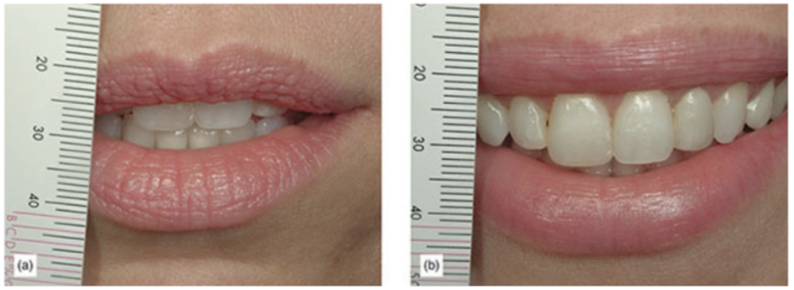
Figure 12: (b) Compare the amount of tooth shown when smiling.
12 Axial Inclination and Rotation (Front Retracted View)
The axial inclination (Figure 13) and rotation [1] are important parameters. They can easily make a smile look less attractive, and the patient should be involved in deciding whether restorative dentistry, preprosthetic orthodontic or orthodontic treatment may be the correct option to correct these discrepancies (Figure 14a-c).
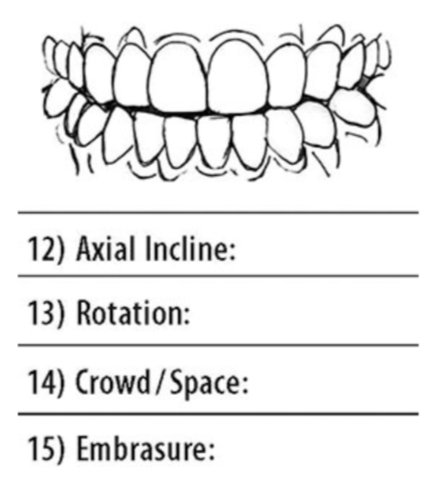
Figure 13: Close up of form with close retracted view.

Figure 14: (a) Female patient with rotation and axial inclination problems who was unwilling to undergo orthodontics. (b) Using the silicon matrix to ensure separation in the correct area, to achieve correct tooth size. (c) Final result with four veneers.
13 Rotation of teeth
Rotation of teeth is easy to spot, and a decision to correct with orthodontic procedures or by using restorative dentistry with all their benefits and consequences must be discussed with the patient.
14 Spacing/Crowding (Front Retracted View)
Often, spacing and crowding can be corrected with orthodontic therapy alone, while sometimes restorative correction can give fast results, and in some cases a combination of treatments may be required. Understanding the patient’s goals, the timeline desired for results and their budget can help to make a final decision (Figures 15a,b,16a-d).

Figure 15: (a) Spacing was deemed to be possible without orthodontics. (b) Good results achieved with veneers only.

Figure 16: (a) Some cases should be treated with preprosthetic orthodontics to avoid ending up with asymmetries or excessively large centrals. (b) Preprosthetic orthodontics to improve spacing. (c) After bracket removal. (d) Postoperative view.
15 Incisal Embrasures (Front Retracted View)
Incisal embrasures are the silhouette of the teeth and key to esthetic results. Evaluating what type of embrasures currently exist and what type of final embrasures or shape of teeth the patient wishes to have will help to clarify the ultimate results. Using a smile book can be helpful to simplify the patient’s selection (Figure 17a,b).
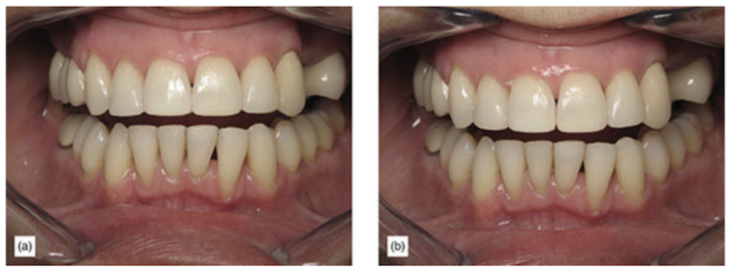
Figure 17: (a) Uneven incisal embrasures can create an undesirable esthetic appearance. (b) Minor enamel recontouring of the incisal edges and embrasures can have a very positive esthetic improvement.
16 Maxillary Anterior Incisor Inclination (Smile Side View)
Maxillary incisors should have a slight forward inclination or proclination to the occlusal plane (Figure 18). Excessive proclination or retroclination is unesthetic, and if the patient finds it undesirable, treatment options including orthodontics must be discussed. Changes on inclination will alter the overjet and must be taken into consideration (Figures 19a-d, 20a,b).
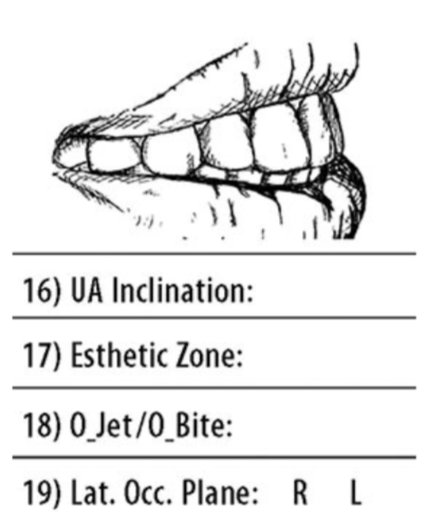
Figure 18: In both retracted and non-retracted lateral views, parameters 16-19 can be evaluated.

Figure 19: (a) Older case of female not wanting wires and brackets orthodontics, which was treated with aggressive tooth preparation for veneers to correct excessive proclination. (b) Final result, lateral view. (c) Front view. (d) Front view of finish veneers, with Invisalign (Align Technology) or MTM Clear Aligner (Dentsply) orthodontics. Aggressive preparation is less desirable and now less common.

Figure 20: (a) Excessive retroclination of anterior teeth. (b) Improved retroclination and effect on lips.
17 Esthetic Zone (Smile Side View)
Because patients usually only view themselves head on, the side photographic views are very revealing and valuable for diagnosis, often making the patient aware of unseen problems and sometimes requiring that restorations extend more distally (Figure 21).

Figure 21: When the patient sees the side-view photographs, they usually see problems they do not see in the usual front mirror view.
18 Overjet and Overbite (Smile Side View and Retracted)
Overjet and overbite are important functional parameters (Figure 22a,b), which sometimes need to be altered to provide the necessary clearance for the envelope of function. It is interesting to realize that many patients think that the ideal position for the teeth is to be border to border, or with minor overjet; they generally see overjet as undesirable. Education at this time is a must to avoid patient dissatisfaction (Figures 23, 24).

Figure 22: (a) 110% overbite and patient biting his palate. (b) After bite opening with bonded veneers and long-term onlay temporaries.

Figure 23: Excessive overjet.

Figure 24: Insufficient overjet.
19 Occlusal Plane from the Lateral View (Smile Side View and Retracted)
It is important to evaluate the occlusal plane from the lateral view. Back teeth should be shorter than front; a reverse plane will have an unesthetic appearance and also has undesirable occlusal consequences (Figure 25a,b).
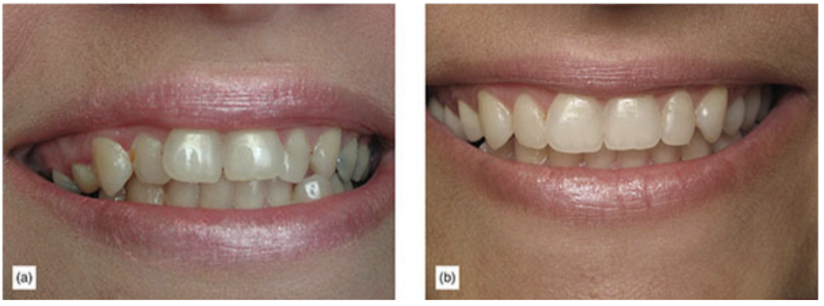
Figure 25: (a) Reversed plane, where the posterior teeth are longer than the anterior with a very unesthetic appearance. (b) Improved reverse plane with a combination of traditional orthodontics and some restorations.
20 Papilla (Front Retracted View)
Papilla (Figure 26a,b), or lack of papilla, can lead to open gingival embrasures, which is a common patient complaint. Acknowledging and developing a treatment plan to correct missing papilla is important. Multiple options with variable results are available, and guided bone regeneration, orthodontic extrusion and restorative options should be discussed. If restorative closure of gingival embrasure is planned, the patient should be aware of the change in the shape of the tooth from a bell shape to a more square shape. Limitations and incomplete closure of the embrasure should be discussed (Figure 27).
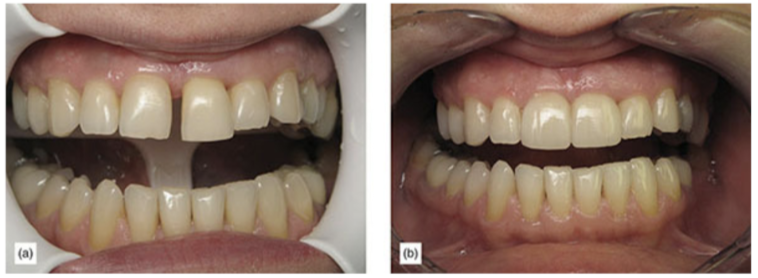
Figure 26: (a and b) Open gingival embrasures and large diastemas can be very challenging.

Figure 27: Gingival zenith of teeth has a great influence in esthetics.
21 Gingival Symmetry (Front Retracted View)
Symmetry of the gingiva is of great esthetic importance when the entire tooth is visible. When the gingiva is visible and there are asymmetries, the patient should be made aware of it and asked if they would like improvement. Based on the severity and the patient’s goals, periodontal correction can be included in the treatment plan.
22 Gingival Biotype (Front Retracted View)
Biotype is important when the esthetic plan includes extractions, implants or fixed partial dentures, or where gingival line stability is important, as it is an important determinant of gingival recession and stability (Figure 28a,b).

Figure 28: Biotype (a) Thin. (b) Thick.
23 Shade (Front Retracted View)
One reason why patients end up unhappy after esthetic treatment is dissatisfaction with the shade of their teeth, and usually they want them to be white. An extremely effective and simple approach is to give the patient two primary options, with a third in special cases: “Natural White” or A1; “Hollywood White” or B1, with a third alternative for younger patients who may already have B1 and are looking for extra white results, “Extra White” or 1M1 — any whiter than this is usually artificial looking (Figure 29a,b).

Figure 29: (a) Teeth dark and stained. (b) After bleaching and veneers.
24 Shape (Front Retracted View)
Tooth shape is not related to the shape of the face [2], but more related to the patient’s preference, gender and age. A simple way to determine the patient’s preference is to use a simple design book, such as the LVI Smile Catalog or the Los Angeles Institute Smile Books.
25 Ratio (Front Retracted View)
Teeth look more symmetrical, and thus more beautiful if the correct ratio of height compared with width is present. This is important mostly when patients show the entire tooth and gum when smiling. Although this is subjective, the approximate ratio is 100% height to approximately 80% width (Figure 30a,b).

Figure 30: (a) The ratio of the teeth makes them look square and anesthetic. (b) After some crown lengthening and veneers.
We hope this article was valuable to you. Our mission is to provide proven, real-world practical techniques, resources, articles and videos to help the community of caring dentists, who value the benefits of minimally invasive Supra-gingival dentistry, expand their knowledge and achieve clinical success, thus giving their patients a healthier form of dentistry.
If you want to delve deeper into Smile Design Using the Dento-Facial Diagnosis System, watch this free video. For updates on newly published articles, courses, and more discussions on Supra-gingival minimally invasive dentistry, sign up to the community.
Sources
- Spear FM. The esthetic correction of anterior dental mal-alignment conventional vs. instant (restorative) orthodontics. J Calif Dent Assoc, 2004; 32(2): 133-141.
- Wolfart S, Menzel H, Kern M. Inability to relate tooth forms to face shape and gender. Eur J Oral Sci, 2004; 112(6): 471-476.
Los Angeles Institute of Clinical Dentistry & Ruiz Dental Seminars Inc. uses reasonable care in selecting and providing content that is both useful and accurate. Ruiz Dental Seminars is not responsible for any damages or other liabilities (including attorney’s fees) resulting or claimed to result in whole or in part, from actual or alleged problems arising out of the use of this presentation. The techniques, procedures and theories on this presentation are intended to be suggestions only. Any dental professional viewing this presentation must make his or her own decisions about specific treatment for patients.