


Source: Supra-Gingival Minimally Invasive Dentistry: A Healthier Approach to Esthetic Restorations, published by Wiley-Blackwell
Direct composite restorations are the most common procedures in restorative dentistry.
However, since many clinicians find direct composites to be complicated, unpredictable, and sometimes unprofitable as third-party compensation is in decline and clinicians deal with extreme fee competition, a time efficient, predictable technique is crucial for the successful and happy professional life of a restorative dentist. Supragingival minimally invasive adhesive techniques make this possible.
A Complicated and Unprofitable Technique?
Most clinicians have complained that direct composite restorations more time consuming and complicated than older techniques such as amalgam, which is often caused by both incorrect techniques and some misunderstanding of restorative material requirements.
One reason why the direct composite restoration procedure can be overcomplicated is that traditional GV black-based techniques of preparations are often being used, followed by a resin-based composite filling. However, the mechanically retentive, geometric GV Black style preparation was designed before adhesion was an option and for different materials.

Figure 1: Geometric amalgam preparation.
Bonded composite, on the other hand, uses materials with special characteristics and a different preparation.
Supragingival minimally invasive adhesive preparations should be simpler and less time-consuming than traditional preparations, which make bonded restorations more complex and unpredictable. An easier filling procedure is facilitated by proper preparation.
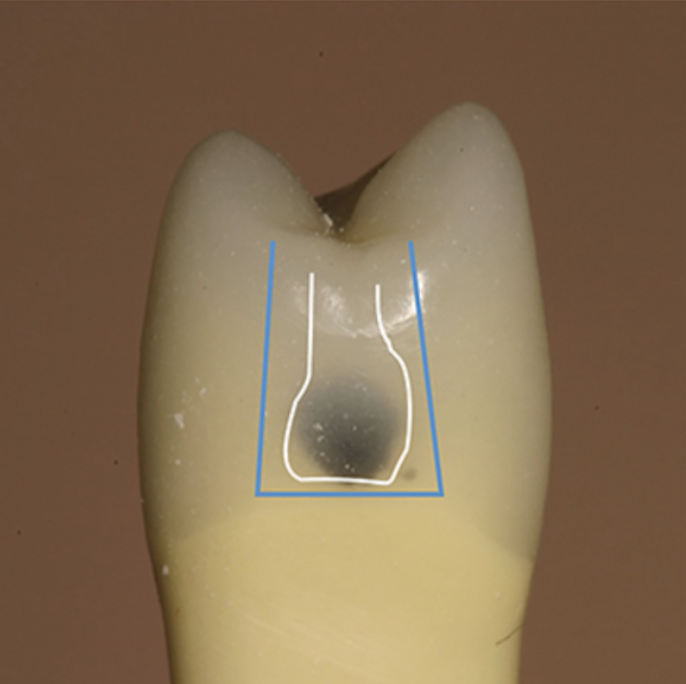
Figure 2: External outline of a traditional geometric preparation vs a bonded composite preparation’s more tooth-preserving outline.
Why Direct Composite Preparations Should Be More Widely Used
Direct composite preparations should be more widely used because:
- Composite does not require bulk for strength unlike amalgam (Figure 3).
- Bonded composite reinforces the tooth structure, including the enamel, eliminating the need to remove a slightly undermined tooth.
- Bonded composites do not require mechanical retention because they rely on adhesives.
- Direct composites are and should be more minimally invasive than traditional restorations.
- Resin-based composite is not tolerant of contamination.
- Subgingival margins are undesirable and lead to higher chances for complications.
- Supragingival protocols shorten and simplify preparation time and make the filling procurement time more predictable.
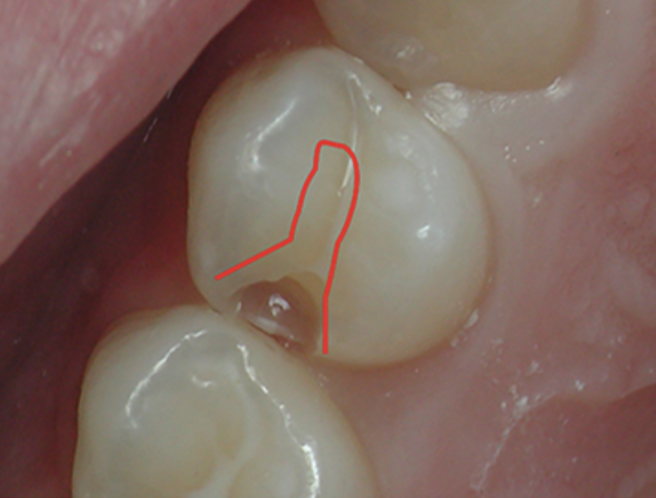
Figure 3: Comparison of a tooth-conserving composite preparation with a traditional occlusal outline (red) for amalgam preparation.
Just as it is important to implement the five principles of supragingival dentistry in indirect procedures, it is equally important to do this during direct restoration procedures. As a reminder, these are:
- Careful removal of old restorations or caries close to the gingiva.
- No boxes or unnecessary retention.
- Enamel preservation and reinforcement.
- Margin elevation.
- Correct use of translucency.
The durability of direct composites has been shown in multicenter studies [1]. In one study that looked at the 5-year durability of composites, it showed a 93% success rate, almost equal to the 95.4% success rate of amalgam [2]. Although very durable, studies have shown very large direct composites fail faster and have shorter durability [3]. With technique improvements, composite durability should be expected to increase.
Multiple studies also fail to prove the superiority of indirect restorations. Some suggest that direct composite outperforms indirect inlays for both composite and porcelain. Indirect restoration should only be performed when there is large damage to the tooth, such as a missing or badly undermined cusp. Indirect inlays are also no more successful or durable than direct composites, and as soon as an inlay is chosen, a taper is needed, which requires more aggressive tooth removal.
Using the proper techniques for direct composites is in the best interest of both the clinical and the patient. Every dentist should be able to perform them with confidence, predictability, and efficiency.
We hope this article was valuable to you. Our mission is to provide proven, real-world practical techniques, resources, articles and videos to help the community of caring dentists, who value the benefits of minimally invasive Supra-gingival dentistry, expand their knowledge and achieve clinical success, thus giving their patients a healthier form of dentistry.
If you want to delve deeper into Direct Composite and learn how using the scientific based supra-gingival approach to preparation and placement allows for highly esthetic, faster, predictable and healthier anterior and posterior direct composites, including full mouth composite rehabilitation, come joining us for our next Direct Composite workshop. For updates on newly published articles, courses, and more, sign up to the community.
Sources
- Gaengler P, Hoyer I, Montag R, Gaebler P. Micromorphological evaluation of posterior composites: A 10-year report. J Oral Rehab, 2004; 32(10): 991-1000.
- Anusavice KJ, Shen C, Rawls HR. Phillips Science of Dental Materials, 12th ed. St Louis, MI: Elsevier Saunders. Da Rosa Rodolpho PA, Cenci MS, Donassollo TA, Loguécio AD, Demarco FF. A clinical evaluation of posterior composite restorations: 17-year findings. J Dent, 2006; 34(7): 427-435.
Los Angeles Institute of Clinical Dentistry & Ruiz Dental Seminars Inc. uses reasonable care in selecting and providing content that is both useful and accurate. Ruiz Dental Seminars is not responsible for any damages or other liabilities (including attorney’s fees) resulting or claimed to result in whole or in part, from actual or alleged problems arising out of the use of this presentation. The techniques, procedures and theories on this presentation are intended to be suggestions only. Any dental professional viewing this presentation must make his or her own decisions about specific treatment for patients.