

Source: Supra-Gingival Minimally Invasive Dentistry: A Healthier Approach to Esthetic Restorations, published by Wiley-Blackwell
Against common belief, traditionally mechanically retained dentistry with subgingival margins is far more complicated than modern supragingival dentistry. But why is this the case? In this article, we will compare the difficulty of mechanically retained dentistry with subgingival margins and supragingival minimally invasive adhesive dentistry.
The Difficulty of Mechanically Retained Dentistry with Subgingival Margins
Traditionally mechanically retained dentistry with subgingival margins is more difficult than modern supragingival dentistry.
For example, a full crown preparation starts with a difficult preparation procedure requiring an exact taper and the need to place a preparation margin subgingivally. When performed correctly in an atraumatic way, the first step requires that an initial equigingival margin and then placement of a retraction cord to expose the subgingival tooth structure. The tooth margin is then prepared (drilled) and placed subgingivally, maintaining a correct taper at all times.
After this difficult procedure, the second cord must be placed to take a proper impression of this subgingival margin, which is also very difficult. In fact, this is one of the most difficult and unsuccessful procedures in dentistry. Laboratories around the country can attest to this due to the amount of inaccurate impressions they receive (Figures 1 & 2a-c) [1].

Figure 1: After the removal of an old bridge, it is easy to see how difficult the tissue management will be, given the deep subgingival margins.

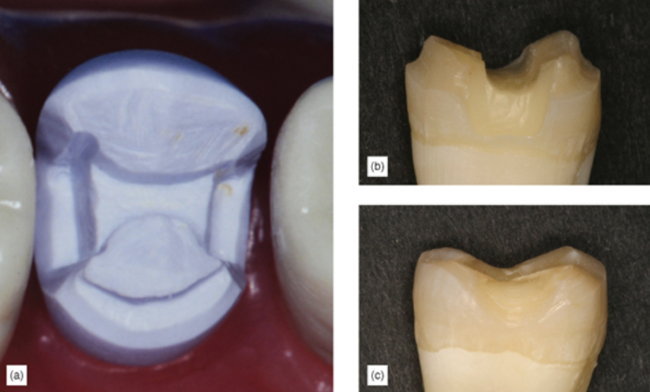
Figure 2: (a) After cord packing, preparations with subgingival margins. (b,c) Even with careful cord packing procedure, observe how blanched and unhealthy the tissue looks.
The cementation procedure is equally difficult. After the provisional is removed from this subgingival preparation, it is not uncommon to see that the gingival is inflamed and bleeds easily (Figure 3). This is usually the consequence of a less than ideal provisional and the patient’s poor oral hygiene. With this bleeding gingiva, hemostasis is difficult for cementation. Additionally, it is not uncommon to see the gingiva grow over the preparation, making proper seating of the restoration difficult without aggressive cord packing (Figure 4a,b). Cement removal is difficult and unpredictable with subgingival margins, and long-term periodontal trauma can be caused by excess residual cement that is not removed (Figure 5).

Figure 3: Gum after removal of the temporary restoration.

Figure 4: (a) Gingival growing over preparation. (b) After removal of the temporary restoration, inflamed gums can be seen growing over preparation.

Figure 5: Crown showing deep margins with cement.
Subgingival margins are no easier with direct restorations. When using resin composite materials and adhesives, subgingival preparation margins have great disadvantages because, once we work subgingivally, bleeding and moisture control are very difficult, additionally, it is harder to place matrix bands and wedges with subgingival margins. Finishing and polishing are also considerably more complicated when margins are subgingival (Figures 6, 7).

Figure 6: Poor margin on deep subgingival class II on first maxillary molar 3, and poor crown margin on lower molar, with bad periodontal consequences.

Figure 7: Multiple deep margin on a class II composite, showing overhangs, sub-margins, open margins and excess material left behind. Deep subgingival margins are difficult to trim and finish.
Supragingival Minimally Invasive Adhesive Dentistry is Easier
Traditional restorative techniques such as full crowns might be thought to be easier compared to partial coverage bonded restorations. However, the opposite is true: keeping margins supragingival is key to simple bonded restorations.
Preparing the tooth for supragingival bonded restoration is significantly simpler. The need for exacting mechanical retention features such as axial reduction with correct taper, and exact boxes, shoulders and offsets during preparation, is eliminated, as adhesive retention is predictable and does not require any retention or resistance forms, greatly simplifying the preparation process (Figure 8 a-c). Also eliminated is the difficult atraumatic subgingival margin placement technique.
The above reasons make supragingival adhesive dentistry preparations simpler and faster to perform correctly compared to traditional crown preparations (Figure 9a,b) [2,3]. Proper preparation leads to easy cementation when the restoration margins are kept supragingival, and the use of a targeted supragingival protocol ensures that the risk of contamination while cementing or bonding is virtually eliminated.

Figure 8: (a) Traditional mechanically retained onlay preparation, showing the exact angles, boxes needed for retention. (b) Compare the greater tooth removal required for a mechanically retained onlay with (c) bonded onlay preparation, demonstrating increased simplicity and tooth preservation.

Figure 9: Comparison of (a) crown preparation with (b) veneer preparation.
Taking an impression of a subgingival margin is one of the most challenging procedures dentists perform (Figure 10a,b) [4,5,6]. Since subgingival margins are equally difficult to reproduce with digital scanners, digital impressions also greatly benefit from supragingival margins (Figure 11a,b). Supragingival restorative techniques make the task of taking impressions easy, making every ensuing step more predictable.

Figure 10: (a) Double cord needed for a crown impression. (b) Even in cases involving more than one tooth, supragingival margins yield an easy impression without a cord.

Figure 11: (a) It is equally difficult to capture subgingival margin detail with a digital impression. With polyvinyl siloxane impression material, it is sometimes virtually impossible (courtesy of Dr Renee Kurtz). (b) Digital impressions are easy with supragingival margins (courtesy of Dr Renee Kurtz).
Temporaries are easier to make when margins are kept above the gingival level because the margins are clear and visible. Temporary cementation can easily be done on a clean, uncontaminated tooth, and the removal of the temporary cement is easy and predictable, allowing for better results and leaving healthier gingiva at the time of permanent cementation (Figure 12a,b).

Figure 12: (a) Provisional on a crown with unhealthy gums. (b) After the provisional is removed, the gums are healthy.
Final cementation also becomes predictable and stress free because there is less room for human error with a more accurate supragingival impression, restorations tend to fit better. There is no need to worry about tissue inflammation, uncontrolled bleeding or placing cord for final cementation because supragingival temporary restorations allow for healthy tissues (Figures 13, 14). Margins are away from the gingival tissues, so bonded cementation is cleaner, easier and more successful. Excess cement is more readily visible, making it easier to remove. Since restorative margins are also more accessible, finishing them is easier and leads to better results (Figure 15). This is true with direct and indirect restorations.

Figure 13: Onlay preparation with supragingival margins are easy to isolate and cement.

Figure 14: Veneer preparation with supragingival margins are easy to isolate and cement.

Figure 15: Inflamed gingival on crowns.
We hope this article was valuable to you. Our mission is to provide proven, real-world practical techniques, resources, articles and videos to help the community of caring dentists, who value the benefits of minimally invasive Supra-gingival dentistry, expand their knowledge and achieve clinical success, thus giving their patients a healthier form of dentistry.
For updates on newly published articles, courses, and more, sign up to the Ruiz Dental Seminars newsletter.
Disclaimer: Los Angeles Institute of Clinical Dentistry & Ruiz Dental Seminars Inc. uses reasonable care in selecting and providing content that is both useful and accurate. Ruiz Dental Seminars is not responsible for any damages or other liabilities (including attorney’s fees) resulting or claimed to result in whole or in part, from actual or alleged problems arising out of the use of this presentation. The techniques, procedures and theories on this presentation are intended to be suggestions only. Any dental professional viewing this presentation must make his or her own decisions about specific treatment for patients.
Sources
- Christensen GJ. The state of fixed prosthodontic impressions: room for improvement. J Am Dent Assoc, 2005; 136(3): 343-346.
- Christensen GJ. Are tooth color onlays viable alternatives to crowns? Clin Rep, 2012; 5(1): 1,3.
- Ruiz JL, Christensen GJ. Myths vs. realities. State of the art indirect posterior restorations. J Cosmetic Dent, 2011; 27(3): 63-72.
- Christensen GJ. Porcelain fused to metal vs nonmetal crowns. J Am Dent Assoc, 1999; 130(3): 409-411.
- Christensen GJ. The state of fixed prosthodontic impressions: room for improvement. J Am Dent Assoc, 2005; 136: 343-346.
- Feng J, Aboyoussef H, Weiner S, Singh S, Jandinski J. The effect of gingival retraction procedures on periodontal indices and crevicular fluid cytokine levels: a pilot study. J Prosthodont, 2006; 15(2): 108-112.