

Source: Supra-Gingival Minimally Invasive Dentistry: A Healthier Approach to Esthetic Restorations, published by Wiley-Blackwell
Mechanically Retained Dentistry with Subgingival Margins is Less Predictable and Less Durable
Because of the long history of crowns and of traditional restorative procedures and rules, it is easy to believe that these procedures are better and more predictable. It is fair to say that almost any procedure, if performed by a master operator, will yield exceptional results. Nevertheless, there are procedures and techniques that are easier to reproduce, and some that are very difficult to reproduce successfully. Traditional crown procedures, such as atraumatic subgingival margin placement, cord packing, subgingival impression, subgingival cementation cleanup and finishing, are among the most difficult and rarely successful procedures in dentistry. The fact that some of these crowns stay on the tooth for some years past their healthy life, does not mean they are successful. In the long term, leaky ill-fitting margins will damage the tooth and the periodontium, and the dentition will have a shorter, less healthy life (Figure 1, 2a,b) Furthermore, microleakage and recurring caries often go undetected with the more traditional opacious materials (PFM and full zirconia), as opacity make it difficult to discover caries visually, and microleakage and radiopacity make it difficult to assess them radiographically.

Figure 1: After crown removal, what was left of the tooth was not sufficient for a restoration.

Figure 2: (a,b) Crown failure needing root removal.
Traditional class II and III restorations with boxes, retentive features, and traditional restorative rules which lead to subgingival margins become exponentially more difficult as the margins become more subgingival. Placing matrix (predictably bonding, filling, finishing, and polishing) becomes extremely difficult. Subsequent chapters discuss techniques to minimize and almost eliminate the need for subgingival margins.
Traditional preparation which requires axial wall, boxes, shoulders, and other mechanical retentive features, requires more tooth removal, leads to increasing closeness to the pulp, and increases heat and damage to the pulp. This can increase the need for root canal therapy on teeth treated with crowns, shortening the life of the restoration and the tooth (Figures 3, 4) [1,2,3,4]. The end result of this is more postoperative pain, unhappy patients, and ultimately, decreased predictability and longevity. Shorter esthetic life increases the chances of pulpal reaction and necrosis, increases periodontal damage, and limits the ability to repair or replace in a timely fashion. With all of these disadvantages, traditional full crowns can hardly be considered successful, predictable or long-lived, even if they can stay in the mouth for many years, well beyond their healthy stage.

Figure 3: There are many little holes on this crown, showing the usual unforeseen common consequence of aggressive preparation.

Figure 4: Two gold crowns with root canal treatment access holes.
Supragingival Minimally Invasive Adhesive Dentistry Is More Predictable and Long Lasting
Many elements must be considered when assessing the real durability of a restoration, the tooth and surrounding tissues. The same supragingival techniques which make the restoration easier, healthier and more esthetic also allow for more predictable, longer-lasting dentistry.
The literature related to the durability of partial coverage bonded onlays and veneers is replete with longevity studies showing excellent results with bonded onlays and veneers, especially when the correct techniques are used. Ruiz and Christensen [5] among other research studies, have shown excellent durability with partial coverage minimally invasive restorations [6,7,8,9,10]. It is my opinion and experience that when using supragingival minimally invasive techniques, the longevity and health of this restoration and surrounding structures can easily outperform any traditional techniques (5a,b). When it comes to longevity, it is important to take occlusion into consideration [11,12]. Occlusion is also a large factor in preventing sensitivity and adverse pulpal responses.

Figure 5: (a) Rehabilitation using bonded onlays and veneers in a case with severe wear. (b) The same tooth over 16 years postoperatively.
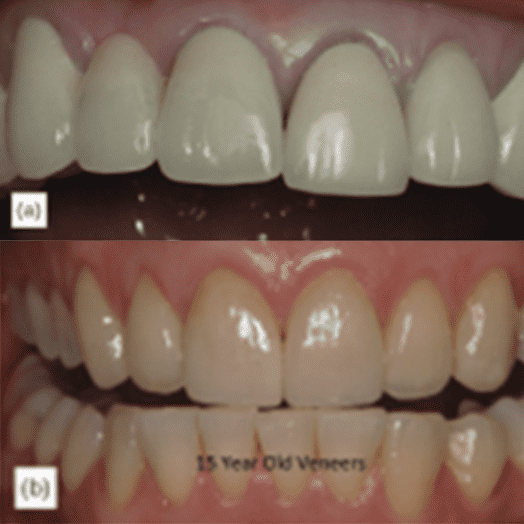
The short esthetic life of the opacious restorations with subgingival margins is a real problem in dentistry [13] because many restorations in the esthetic zone are replaced, not because of clinical failure but because after the gingiva recedes, the unsightly margin is exposed and the restoration must be replaced. This problem can be avoided altogether by using proper translucency and supragingival techniques. This in fact lengthens the life of restorations in the esthetic zone (Figure 6a,b).

Figure 6: (a) The patient was unhappy with gray margins, and requested replacement with clinically acceptable crowns. (b) Veneers at 15 years postoperatively; the margins are visible, but the patient is still happy with this esthetic look.
Patient satisfaction is part of predictable success. Patients do not like to think that their tooth is being drilled down to a nub. When a patient is educated about minimally invasive procedures, they find them to be reassuring and comforting. Equally positive responses from patients are attained when educating them about the benefits of not invading their gingival sulcus and allowing the gingiva to stay healthy using supragingival techniques.
Reparability enhances the longevity of bonded restorations dramatically. Restorative materials such as porcelain and composite can be repaired intraorally with great predictability [13], rather than replacing them (Figures 7a-c). In most cases, a repair will add many years of additional service to a restoration.

Figure 7: (a) A fracture on the distolingual cusp of a ceramic onlay after 10 years. (b) Porcelain repair. (c) The repair will serve the patient a few more years.
Traditional restorative techniques with subgingival margin placement and opacious materials hide secondary caries and marginal leakage, which, in the long term, will allow for irreparable damage to occur. The use of non-metal translucent restorative materials, which blend better at the cavosurface margin area, not only allows for better esthetic results, but also allows the clinician to leave the margin above the gum. When recurring caries or marginal leakage occurs, as it does with all types of restorations, the problem is easier to distinguish in an x-ray of a metal-free restoration. This allows for an earlier intervention. The ability to easily identify caries early and repair or replace the restoration prevents unnecessary root canal work, extensive secondary caries and sometimes the complete loss of a tooth, once again showing supragingival dentistry as the healthier option for the patient.
Regarding durability, it is important to consider not only the durability of the restoration, but also the durability of the surrounding structures. What is more important: the longevity of the restoration, the longevity of the tooth, or both? Of course, patients and dentists would want both to last as long as possible. Undoubtedly, on the larger scale, the longevity of the tooth itself is most important, as that is the ultimate goal. Supragingival minimally invasive bonded restorations are the best choice when considering the health of the restoration and the surrounding tissues.
We hope this article was valuable to you. Our mission is to provide proven, real-world practical techniques, resources, articles and videos to help the community of caring dentists, who value the benefits of minimally invasive Supra-gingival dentistry, expand their knowledge and achieve clinical success, thus giving their patients a healthier form of dentistry.
For updates on newly published articles, courses, and more, sign up to the community.
Disclaimer: Los Angeles Institute of Clinical Dentistry & Ruiz Dental Seminars Inc. uses reasonable care in selecting and providing content that is both useful and accurate. Ruiz Dental Seminars is not responsible for any damages or other liabilities (including attorney’s fees) resulting or claimed to result in whole or in part, from actual or alleged problems arising out of the use of this presentation. The techniques, procedures and theories on this presentation are intended to be suggestions only. Any dental professional viewing this presentation must make his or her own decisions about specific treatment for patients.
Sources
- Thomas MS, Kundabala M. Pulp hyperthermia during tooth preparation: The effect of rotatory instruments, laser, ultrasonic devices and airborne particle abrasion. J Calif Dent Assoc, 2012; 40(7): 571-576.
- Davis GR, Tayeb RA, Seymour KG, Cherakara GP. Quantification of residual dentine thickness following crown preparation. J Dent, 2012; 40(7): 571-576.
- Dahl BL. Dentine/pulp reactions to full crown preparation procedures. J Oral Rehabil, 1977; 4(3): 247-254.
- Langeland K, Langeland LK. Pulp reactions to cavity and crown preparation. Aust Dent J, 1970; 5(4): 261-276.
- Ruiz JL, Christensen GJ, Sameni A, Vargas L. Clinical performance of bonded ceramic and resin-based composite inlays and onlays using a self-etch bonding system; a 51-month report. Inside Dentistry, 2007; 3(5): 62-65.
- Gresnigt M, Ozcan M. Esthetic rehabilitation of anterior teeth with porcelain laminates and sectional veneers. J Can Dent Assoc, 2011; 77:b143.
- Van Dijken JW, Hasselrot L. A prospective 15-year evaluation of extensive denti-enamel-bonded pressed ceramic coverage. Dent Mater, 2010; 26(9): 929-939.
- Land MF, Hopp CD. Survival rates of all ceramic systems differ by clinical indication and fabrication method. J Evid Based Dent Pract, 2010; 10(1): 37-38.
- Gurel G. Clinical performance of porcelain laminate veneers: outcomes of the aesthetic pre-evaluative temporary (APT) technique. Int J Periodont Restorative Dent, 2012; 32(6): 625-635.
- Gurel, G. Influence of enamel preservation on failure rates of porcelain laminate veneers. Int J Restorative Dent, 2013; 33(1): 31-39.
- Ruiz JL. Occlusal disease: restorative consequences and patient education. Dent Today, 2007; 26(9): 90-95.
- Ruiz JL. Achieving longevity in esthetics by proper diagnosis and management of occlusal disease. Contempt Esthet, 2007; 11(6): 24-27.
- Christensen GJ. Porcelain fused to metal vs nonmetal crowns. J Am Dent Assoc, 1999; 130(3): 409-411.